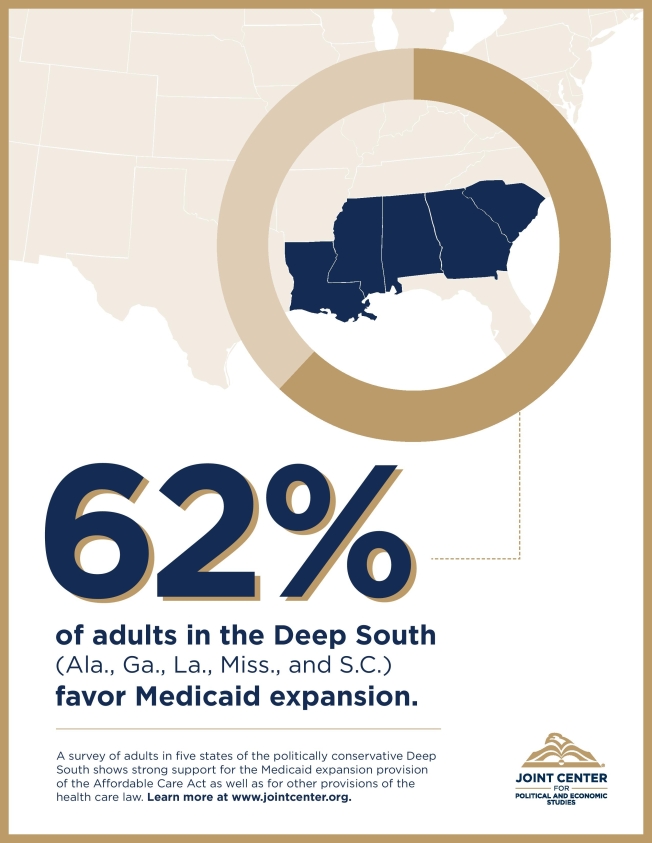
Click the image to read our newest report, “The Deep South and Medicaid Expansion: The View From Alabama, Georgia, Louisiana, Mississippi, and South Carolina,” and learn more about public perception of the Affordable Care Act.
Click the image to read our newest report, “The Deep South and Medicaid Expansion: The View From Alabama, Georgia, Louisiana, Mississippi, and South Carolina,” and learn more about public perception of the Affordable Care Act.
In February, the U.S. Food and Drug Administration (FDA), through its accelerated approval regulations, approved and granted exclusivity to KV Pharmaceuticals to market Makena (17Alpha Hydroxyprogesterone Caproate). The drug is also known as 17P, a synthetic hormone delivered by weekly intramuscular injection to slow the progression of pre-term birth (PTB) before 37 weeks of pregnancy, among pregnant women with at least one previous spontaneous PTB. Although the drug is not for use for women with other risk factors for PTB or women pregnant with twins, it has been sold for years without approval. Today, the drug just comes with a large price tag.
PTB is one of the leading causes of neonatal mortality in the United States. Major risk factors for PTB include behavioral and demographic characteristics such as race/ethnicity, maternal age, history of preterm delivery, stress, income, education, employment, housing, prenatal care utilization, smoking, alcohol consumption and marital status. Already, the preterm birth rate is roughly 13 percent of live births, accounting for 500,000 infant deaths annually.
On March 14, 2011 the new 17P, Makena was officially brought to market, marking the first FDA approval of a drug for the prevention of PTB. Subsequently, the prescription cost increased from $20 to $1500 per dose. Recent studies support the use of progesterone supplementation for patients at risk for PTB. The American College of Obstetricians and Gynecologists (ACOG) has promoted the use of 17P injections since 2003, following two successful randomized placebo-controlled trials. Research has shown that approximately one-third of pregnant women receiving weekly 17P injections have had successful outcomes resulting in the prevention of PTB. And in 2008, ACOG issued a Committee Opinion indicating that progesterone for the prevention of PTB should be offered to women with a history of spontaneous PTB.
Some obstetricians, maternal health and public health practitioners, including family planning advocates, are outraged at the dosage price increase for 17P and have spoken out and written letters to KV. As a result, the St. Louis drug company has been criticized for increasing the price of Makena. In April, the company announced that it would cut the price by more than half (in fact KV reduced the dosage price to $690 two days after the FDA publicly invited competition by announcing that it would continue to allow compounding pharmacies to make and sell a generic version of the drug). Now, instead of a pregnancy costing $30,000, a much improved price of $13,800 will make the drug more accessible.
During one of the first opportunities that I had to present testimony at a Congressional hearing, a member of the committee posed a challenging question to me and other witnesses at our panel: Would you trade your current health insurance for Medicaid?
The Congressman’s intent was clear: he and others who oppose expansions of public health insurance programs believe that Medicaid is worse than private insurance, and possibly even worse than no insurance at all.
I was the first witness seated on the right of the panel, so I was to respond first. I hesitated. I didn’t want to reinforce the idea that Medicaid was deeply flawed. Sure, the program has problems, but it remains one of the most efficient health insurance programs in the country and has been a lifeline for millions of low-income and disabled Americans. But trade the insurance I had at the time? I caved and answered no. Almost all of the witnesses at our panel did the same. But I’ve regretted it since.
Yesterday a landmark new study was released that, for the first time, documents the many ways in which Medicaid improves the health and well-being of its beneficiaries. Researchers found that “expanding low-income adults’ access to Medicaid substantially increases health care use, reduces financial strain on covered individuals, and improves their self-reported health and well-being.” The study was remarkable because for the first time researchers were able to compare outcomes for people who were randomly assigned to Medicaid against those who sought Medicaid coverage but could not receive it due to budget constraints. (http://www.hsph.harvard.edu/news/press-releases/2011-releases/medicaid-benefits-oregon-study.html)
The implications of the study are clear: efforts to slash Medicaid, such as those being debated in Congress, would increase risks for poor health and financial ruin for millions of children, elderly, and/or disabled people. These are the very folks who are struggling the most in the current economy. And given the high cost of poor health for our nation as a whole, these cuts are not only morally wrong but also put our economic recovery at risk.
Medicaid works. Let’s spread the word. I wish I had when I was given the chance to correct the record.
Welcome to the blog of the Joint Center for Political and Economic Studies. The Joint Center for Political and Economic Studies informs and illuminates the nation’s major public policy debates through research, analysis, and information dissemination in order to: improve the socioeconomic status of African Americans and other minorities; expand their effective participation in the political and public policy arenas; and promote communications and relationships across racial and ethnic lines to strengthen the nation’s pluralistic society.
This blog serves to keep the public abreast of our research and analysis of current and proposed policy, activities and events around the country, as well as major decisions facing the national and local governments. Through the Health Policy Institute, Media and Technology Institute, and Climate Change Initiative, the Joint Center is working around the clock to illuminate these issues as they pertain to communities of color, and expound upon possible solutions.
